Donepezil did not reduce the rate of
institutionalisation or disability in people with mild to moderate Alzheimer’s
disease
Setting:
22 hospitals in the UK; October 1998 to
September 2001.
Patients:
565 people (median age 75 years, range
46–93 years) with mild to moderate Alzheimer’s disease (DSM-IV). Main exclusion
criteria: living in an institution, no regular carer, contraindications against
donepezil, or already receiving cholinesterase inhibitors.
Intervention:
Run-in treatment: donepezil (5
mg/day) or placebo for 12 weeks. Long term treatment: donepezil (5 or
10 mg/day) or placebo for 48 weeks. (The intervention continued with a 6 week
washout; then two rounds of donepezil (5 or 10 mg/day) or placebo for 48 weeks
followed by 4 weeks washout; however, these results not reported due to high
dropout rate).
Outcomes:
Entry into institutional care;
progression of disability (Bristol Activities of Daily Living (BADLS)).
Patient follow up:
75% for placebo, 76% donepezil (see
notes) at 60 weeks.
MAIN RESULTS
At 60 weeks, there were no significant
differences between donepezil and placebo in institutionalisation rates or
progression to disability in people with mild to moderate Alzheimer’s disease
(see http://www.ebmentalhealth.com/supplemental for table). There
were no significant differences in institutionalisation rates between the 10 mg
and 5 mg donepezil groups (10 mg v 5 mg: 37 v 44, p = 0.7).
CONCLUSIONS
Donepezil does not delay time to
institutionalization or progression to disability in people with mild to
moderate Alzheimer’s.
Donepezil은
경증에서 중등도의 알츠하이머 병 환자에게 제도화 또는 장애율을 감소시키지 않았습니다.
환경:
영국의 22
개 병원; 1998
년 10
월 ~
2001 년 9
월
환자 :
경증 내지 중등도의 알츠하이머 병 (DSM-IV)을
가진 565 명
(중간
연령 75 세, 46-93 세
범위). 주요
배제 기준 : 기관에서의
생활, 정기적
인 간병인, 도네
페질에 대한 금기 또는 이미 콜린 에스테라아제 저해제 투여.
개입 :
중재 치료 : 12
주 동안 donepezil
(5mg / day) 또는 위약. 장기
치료 : donepezil (5 또는 10mg
/ day) 또는 위약을 48
주 동안 사용하십시오. (중재는 6
주간의 유실로 이어지고, 48 주간
도네 페질 (5 또는
10mg / day) 또는 위약 2
회 2
회 접종 후 4
주간의 유실이 있었지만,이
결과는 높은 유실율로보고되지 않았다.
결과 :
제도적 관심 사항; 장애 진행 (Bristol
Activities of Daily Living (BADLS)).
후속 조치 :
위약 75
%, 도네 페질 76
% (주 참조).
주요 결과
60 주에, 알츠하이머
병이 경증에서 중등도의 사람들에서 제도화 속도 또는 장애로 진행되는 도네 페질과 위약 간에는 유의 한 차이가 없었다 ( http://www.ebmentalhealth.com/supplemental 참조 ). 10mg과 5mg의 도네 페질 그룹 (10mg v 5mg
: 37 v44, p = 0.7) 간에는
제도화 율에 유의 한 차이가 없었다 .
결론
Donepezil은
가벼운 알츠하이머 병 환자와 중증 알츠하이머 병 환자의 장애로의 진행을 지연시키지 않습니다.
출처 :
http://ebmh.bmj.com/content/7/4/112
Long-term donepezil treatment in 565
patients with Alzheimer's disease (AD2000): randomised double-blind trial.
Abstract
Cholinesterase inhibitors produce small
improvements in cognitive and global assessments in Alzheimer's disease. We
aimed to determine whether donepezil produces worthwhile improvements in
disability, dependency, behavioural and psychological symptoms, carers'
psychological wellbeing, or delay in institutionalisation. If so, which
patients benefit, from what dose, and for how long?565 community-resident
patients with mild to moderate Alzheimer's disease entered a 12-week run-in
period in which they were randomly allocated donepezil (5 mg/day) or placebo.
486 who completed this period were rerandomised to either donepezil (5 or 10
mg/day) or placebo, with double-blind treatment continuing as long as judged
appropriate. Primary endpoints were entry to institutional care and progression
of disability, defined by loss of either two of four basic, or six of 11
instrumental, activities on the Bristol activities of daily living scale
(BADLS). Outcome assessments were sought for all patients and analysed by logrank
and multilevel models.Cognition averaged 0.8 MMSE (mini-mental state
examination) points better (95% CI 0.5-1.2; p<0.0001) and functionality 1.0
BADLS points better (0.5-1.6; p<0.0001) with donepezil over the first 2
years. No significant benefits were seen with donepezil compared with placebo
in institutionalisation (42% vs 44% at 3 years; p=0.4) or progression of
disability (58% vs 59% at 3 years; p=0.4). The relative risk of entering
institutional care in the donepezil group compared with placebo was 0.97 (95%
CI 0.72-1.30; p=0.8); the relative risk of progression of disability or
entering institutional care was 0.96 (95% CI 0.74-1.24; p=0.7). Similarly, no significant differences
were seen between donepezil and placebo in behavioural and psychological
symptoms, carer psychopathology, formal care costs, unpaid caregiver time,
adverse events or deaths, or between 5 mg and 10 mg donepezil.Donepezil is not
cost effective, with benefits below minimally relevant thresholds. More
effective treatments than cholinesterase inhibitors are needed for Alzheimer's
disease.
알츠하이머 병 환자 565 명 (AD2000)의 장기간의 도네 페질 치료 : 무작위 이중 맹검 시험
요약
콜린 에스테라아제 억제제는 알츠하이머 병의인지 및 전반적인 평가에서 작은
향상을 가져옵니다. 우리는
도네 페질이 장애, 의존, 행동
및 심리적 증상, 간병인의
심리적 안녕 또는 제도화의 지연을 보완 해 줄지 여부를 결정하고자했습니다. 그렇다면 어떤 환자가 어떤 용량으로 어떤 용량으로 얼마 동안 그리고 얼마나
오랫동안 혜택을 받는가? 알츠하이머 병이 경증에서 중등도에 이르는 지역 사회 거주자 환자는 무작위로
도네 페질 (5mg / day) 또는 위약. 이 기간을 마친 486
명의 환자는 donepezil
(5 또는 10mg
/ day) 또는 위약으로 재조정되었고, 이중
맹검 법으로 적절한 것으로 판단된다. 1
차 평가 변수는 제도적 관심과 장애 진행으로 이어졌으며, (BADLS)의 브리스톨 활동에 대한 4 가지
기본 또는 6 가지
중 11 가지
수단 중 2 가지
중 하나가 손실 됨으로 정의됩니다. 모든 환자에 대해 결과 평가가 이루어졌고 logrank 및
multilevel 모델로
분석되었습니다. 인식은
평균 0.8 MMSE (미니
정신 상태 검사) 포인트
(95 % CI 0.5-1.2; p <0.0001)와 기능성 1.0
BADLS가 더 좋음을 나타냅니다 (0.5-1.6 p <0.0001)를 처음 2
년 동안 도네 페질과 비교 하였다. 도네
페질은 위약과 비교하여 도네프 화제 치료에 비해 유의미한 효과가 없었다 (3
년 44
% 대 44
%, p = 0.4) 또는 장애
진행 (3 년
59 %, p = 0.4). 도네 페질 군에서 위약군에 비해 제도적 치료를받을 위험은 0.97 (95 % CI 0.72-1.30; p = 0.8); 장애 진행 또는 제도 진료의 상대적 위험은 0.96 (95 % CI 0. 74-1.24; p =
0.7). 마찬가지로, 행동
및 심리 증상, 간병인
정신 병리학, 공식
간호 비용, 무보수
간병인 시간, 부작용
또는 사망, 또는
5 mg에서 10 mg의
도네 페질간에 도네 페질과 위약 사이에는 유의 한 차이가 없었습니다. 최소 관련 임계 값 이하. 알츠하이머 병에 콜린 에스테라아제 억제제보다 효과적인 치료법이 필요합니다.
출처 : Lancet (London, England) [01 Jun 2004, 363(9427):2105-2115]
http://europepmc.org/abstract/med/15220031
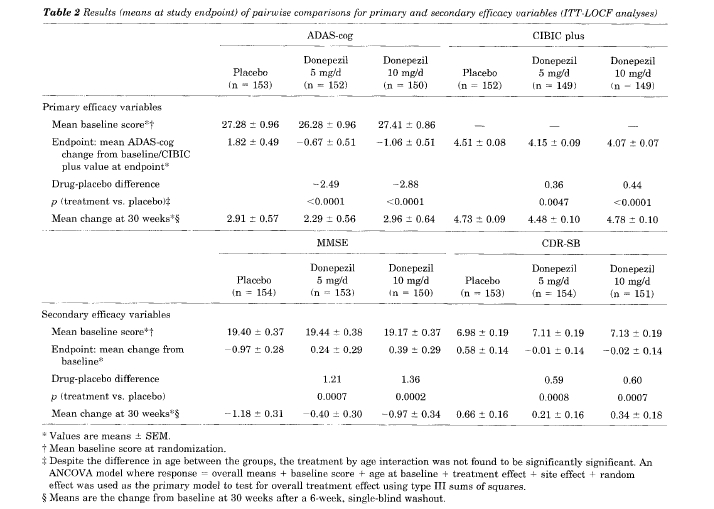
A 24=week, double-blind, placebocontrolled trial of donepezil in patients with Alzheimer’s disease
S.L. Rogers, PhD; M.R. Farlow, MD; R.S. Doody, MD, PhD; R. Mohs, PhD; L.T. Friedhoff, MD, PhD;
and the Donepezil Study Group*:
Article abstract-The efficacy and safety of donepezil as a treatment for patients with mild to moderate Alzheimer’s
disease (AD) was investigated in a multicenter, double-blind study. Patients were randomly assigned to treatment with
placebo (n = 1621, 5 mgld donepezil (n = 154), or 10 mgld donepezil (n = 157) for 24 weeks followed by a 6-week,
single-blind placebo washout. The primary efficacy measures were the cognitive portion of the Alzheimer’s Disease
Assessment Scale (ADAS-cog) and the Clinician’s Interview Based Assessment of Change-Plus (CIBIC plus), with the
Mini-Mental State Examination (MMSE), Clinical Dementia Rating Scale-Sum of the Boxes (CDR-SB), and patient rated
Quality of Life (QoL) used as secondary measures. Cognitive function, as measured by the ADAS-cog, was significantly
improved in the 5- and 10-mgld donepezil groups as compared with the placebo group at weeks 12, 18, and 24. Clinician’s
global ratings on the CIBIC plus also improved in both the 5- and lO-mg/d donepezil groups relative to placebo. At the end
of the 6-week placebo washout phase, ADAS-cog scores and CIBIC plus ratings were not significantly different for the
three groups. Significant treatment benefits were also observed consistently in both the 5- and 10-mgld groups on the
MMSE and the CDR-SB, but there was no consistent effect on the patient-rated QoL. Cholinergic side effects (primarily
diarrhea, nausea, and vomiting) were reported more often in the 10-mgld group than either the 5-mgld or placebo groups.
Side effects were transient and generally mild in severity. These data indicate that donepezil is a well-tolerated drug that
improves cognition and global function in patients with mild to moderate AD.
NEUROLOGY 1998;50:136-145
아리셉트정은 알츠하이머형 치매증상의 치료, 혈관성 치매(뇌혈관질환을 동반한 치매) 증상을 개선하는 약물이다. 현재 국내에 시판중인 치매약은 모두 4가지 제품이 있다. 아리셉트(성분명 도네페질), 엑셀론(리바스티그민), 레미닐(갈란타민), 에빅사(메만틴) 등이다. 아리셉트는 도네페질 오리지널 의약품이다. 일본 제약회사인 에자이가 개발해 국내에서는 1999년부터 대웅제약이 위탁 생산해 판매하고 있다. 2008년 특허가 만료되면서 40여개의 제네릭 제품이 쏟아졌다. 알츠하이머성 치매 증상 완화제는 도네페질 성분의 약물이 대표적이다. 2015년 기준으로 1500억원이 넘는 전체 시장에서 80%를 넘게 점유했다. 한마디로 가장 많이 처방되고 복용하는 약물이다. 그 만큼 타 약물보다 '치료 효과'가 좋다는 방증일 수도 있다.
2016-06-29 06:00:20
출처 : 약사공론
http://www.kpanews.co.kr/article/show.asp?idx=175001&table=article&category=D
아리셉트[Aricept ], 엑셀론[Exelon ], 레미닐[Reminyl]
: “콜린에스테라제 억제제” 계열의 치매 치료제
1970년대 후반, 알츠하이머-병의 환자의 뇌에서는, “아세틸콜린”이라는 신경전달 물질의 양(量)이 감소하고 있는 것이 알려졌다.
아세틸콜린은 뇌(腦)내에서는 기억과 학습 등에 관계하고 있다.
신경말단으로부터 분비되는 전달물질로 운동신경과 부교감신경에서는 아세틸콜린이,
교감신경에서는 에피네프린(아드레날린)이 알려져 있다.
아세틸콜린이 분비되면 혈압강하 ·심장박동 억제 ·장관(腸管) 수축 ·골격근 수축 등의 생리작용을 나타낸다.
신경말단에서 분비된 아세틸콜린은 자극의 전달이 끝나면 콜린에스테라아제에 의해 콜린과 아세트산으로 분해된다.
아리셉트 부작용
| 구분 |
매우 자주 |
자주 |
때때로 |
드물게 |
빈도불명 |
| 감염 |
|
감기 |
|
|
|
| 대사 및 영양 |
|
식욕부진 |
|
|
|
| 정신계 |
|
환각**,흥분**,공격적행동** |
불안증,불면증,졸음,성욕증가
,수다,조증 |
|
악몽,신경과민
,헛소리,망상,우울증 ,혼돈,무관심,운동과다증 |
| 신경계 |
|
실신*,어지러움,불면,진전 |
발작* |
추체외로증상 |
혼미 |
| 심혈관계 |
|
|
서맥,심계항진 |
동방심차단,방실차단 |
고혈압,저혈압,심방세동 |
| 소화기계 |
설사,구역 |
구토,복부장애(복통포함) |
위장관출혈,위십이지장궤양,변비,타액분비 |
|
삼킴곤란,대변실금 |
| 간-담도계 |
|
|
|
간염을
포함한 간 장애*** |
|
| 피부 및 피하조직 |
|
발진,가려움증 |
|
|
|
| 근골격계, 접합 조직 및 뼈 |
|
근육
경련 |
|
|
근육통 |
| 신장 및 비뇨기계 |
|
요실금 |
|
|
빈뇨,요정체 |
| 전신 및 투여 부위 |
두통 |
피로,통증,치통 |
안면홍조,권태감,무기력증 |
|
부종(안면부종
포함),발열 ,체온감소 |
| 혈액계 |
|
헤마토크리트감소 |
백혈구감소증 |
|
빈혈,혈소판감소증 |
출처
http://terms.naver.com/entry.nhn?docId=2129763&categoryId=51000&cid=51000
|
;)